
Background
As many of my readers know, in early 2020 I was diagnosed with prostate cancer. For more details about my initial diagnosis, you can read this article.
To make a long story short, I didn’t like the long term consequences of the treatment options my doctor gave me. For me, being alive is more than just having a heart beat. I didn’t want to live a life with the inability to ever have sex again, urinary incontinence, and potential bowel and bladder damage from radiation or surgery. I chose not to treat my cancer.
My doctors told me that if I didn’t have surgery or radiation treatments within about six months of my diagnosis, the cancer would most certainly spread. The docs gave me a projected life expectancy of two years if I didn’t treat the cancer.
In late 2022, a reader contacted me and told me about a newly-approved treatment option. The TULSA PRO trans-urethral total prostate ablation procedure wasn’t commonly available in the United States when I was diagnosed. None of my docs even mentioned it as a possible option. By 2022, the procedure was becoming more widely known and performed. My reader had undergone the TULSA. His cancer was gone and he had no urinary or sexual side effects.
That interested me. As my PSA levels continued to rise and my MRIs showed that my cancer was nearly breaking out of the prostate, I booked an appointment with Dr. Busch to have the Tulsa procedure done.
The whole prostate ablation was a relatively easy recovery. Other than having a catheter for 11 days and a six-week restriction on sex and heavy lifting, the recovery wasn’t bad at all. My first followup MRI showed that the doc got all the cancer. I could still have sex and I had zero urinary issues. Life was good for about a year and then my PSA started rising again. Fourteen months after the TULSA procedure, my cancer came back and spread to some pelvic lymph nodes.
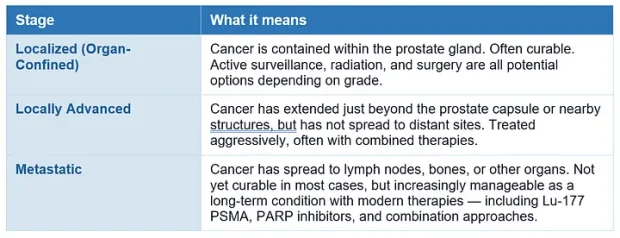
Now my cancer was at stage IV and was no longer considered curable. The definitive treatment was taking my testosterone down to zero for the rest of my life. That would stop the cancer growth for a few years, but would eventually stop working. And those few years with zero testosterone wouldn’t be a life I would consider living. I again chose not to treat my cancer.
About a year later (last summer) I was in bad shape. I had horrific nausea and couldn’t eat. I lost 30 pounds in two months. I was in horrible pain from one of my tumors pressing on a nerve in my lower back. I couldn’t teach a class without stepping off the range to vomit several times a day. I thought I was going to have to stop teaching.
At that point, I tried some experimental treatment protocols. Those protocols shrunk my tumors and drastically lowered my PSA. All my docs were astounded. They had never seen any treatments work as well as my experimental protocols did.
Unfortunately, I’m a bit of an outlier. I know three other prostate cancer patients who tried protocols similar to the one I used to reduce my tumor size. The protocol caused some temporary progress, but ultimately failed in all three of the other guys who tried it.
Right now I feel good and my PSA numbers are much better than they were at this time last year. I just don’t know how long my reprieve will last. I still have the cancer, it just doesn’t seem to be growing right now.
Median survival from the time of diagnosis of my type of cancer until death is 30 months. And that’s with hormone depletion treatment. I’m not doing hormone treatment and I’m at month 28 since my cancer spread. I feel good now, but I expect that’s temporary. I’m enjoying my life currently, but I don’t expect this remission to last forever.
At this point, a significant percentage of you readers will feel the need to tell me about Ivermectin, Fenbendazole, high dose melatonin, ketogenic diets, Essiac Tea, IV Vitamin C, apricot seeds, Gerson therapy, and some funky clinic in Mongolia that cured your cousin’s friend’s brother’s cancer. Please don’t.
I’ve tried most of the “alternative treatments.” They didn’t work. I’ve been researching treatment options for my condition daily for six years. I’ve been to 11 different doctors and had full cancer workups at both MD Anderson and UCLA. You watched a Tiktok video or heard a podcast. I know you mean well, but it becomes incredibly annoying when I get 200 treatment suggestions from people who have never had my type of cancer every time I write about an update in my condition. Resist the urge to tell me about the surefire cure you just heard about on social media.
So what’s the point of this article?
It isn’t just to update you on my condition. It’s to provide some informed guidance for those of you who might be going through a similar cancer experience.
I look at the quote above and am humbled. In 30+ years of martial arts training, gun classes, and police work, I’ve learned a lot. In essence, I serve as a kind of “survival guide” to all my students and readers.
When I told my late friend Marcus Wynne that I had cancer, he said “You’ve saved a lot of lives with your training over the years. I predict you will save even more lives when you tell people about how you have survived your medical challenges.”
When Marcus told me that, I laughed at him. Now, having helped a whole lot of guys with cancer since my own diagnosis in 2020, I realize Marcus had access to information that most folks couldn’t understand.
Right now I’m being contacted by a couple people every month who have recently been diagnosed with prostate cancer. I’m writing this article to share the stuff I’ve learned over the years about my disease and to tell folks all the stuff I wished I had known when I was going through the initial stages of my diagnosis.
Keep reading if you want some general tips and are interested in the most valuable resources I’ve found to help prostate cancer patients through their disease progressions. This isn’t medical advice. I’m not a doctor. I’m just a patient who has been dealing with this terminal disease for more than six years. I know what has been helpful for me and I want to share those resources with all of you in a similar situation.
General Prostate Cancer Tips
High PSA– For most prostate cancer patients, their first indication of the disease comes after a high PSA. If your PSA blood test comes back high, don’t panic. Almost half of the folks with a high PSA (4.0 or 5.0 depending on age) DO NOT HAVE CANCER. Lots of conditions can raise PSA levels, most commonly BPH and prostatitis.
Any type of pressure on the prostate can also temporarily raise levels. Make sure you don’t have orgasms, heavy lower body workouts, jujitsu classes, or cycling workouts within 72 hours of your PSA test. The most common approach to an initially high PSA level is to wait one to two months and then retest.
MRI- If your PSA remains high, the next step should be an MRI in attempt to locate any lesions or tumors in the prostate. This is a relatively new recommendation. Up until a few years ago, biopsy would be the next steps. Lots of urologists still go with a biopsy before the MRI.
The prostate biopsy is a nasty procedure. You will want to limit the number of biopsies you endure. It’s better to go with the MRI first if your doc will order one.
Biopsy- If the MRI discovers lesions or tumors, a biopsy is warranted. No insurance company will approve cancer treatment based just on MRI results. A diagnosis of prostate cancer via biopsy is the only way you will be approved for treatment. The most common biopsy is called a TRUS biopsy. The doctor divides the prostate into 12 different areas using ultrasound imaging. The doc attempts to get a tissue sample from each of those 12 segments.
Other biopsies use MRI to target specific areas of suspicion rather than randomly taking 12 tissue samples. There is an MRI fusion biopsy that uses a computer and ultrasound to merge MRI results with ultrasound images to better guide the needle sampling. The most accurate biopsy is called an in-bore MRI biopsy. This one is actually done in an MRI machine, but it’s expensive and difficult to schedule.
If I had to do the biopsy stage again, I wouldn’t consent to the random 12 needle TRUS biopsy. I would insist on one of the MRI biopsies of the suspicious areas rather than the random sampling.
There are two ways the biopsy needles are inserted. The most common is trans-rectally. Because there is a lot of bacteria in the rectum, there is a high risk of infection. In most other countries, trans-rectal biopsies are no longer conducted.
The other option is trans-perineal insertion where the needle is inserted into the tissue between the scrotum and the anus. That is slightly more painful, but cuts risk of infection down to almost zero. If you can find a doc who will do a trans-perineal biopsy, that’s what I would recommend.
One other surprising thing about biopsies is that you may find blood in your urine, stool, or ejaculate for a couple weeks afterwards. I had no blood in urine or stool after my first biopsy. I wasn’t expecting my first few orgasms to expel what appeared to be straight blood rather than semen. My girlfriend at the time was even more surprised than I was. Be prepared for that possibility.
Gleason score and review of biopsy slides- A pathologist will review the tissue samples collected in the biopsy and evaluate the grade of cancer you have. That grade is most commonly expressed as a Gleason Score. This Gleason score will dictate all of your future treatment options. It’s really important.
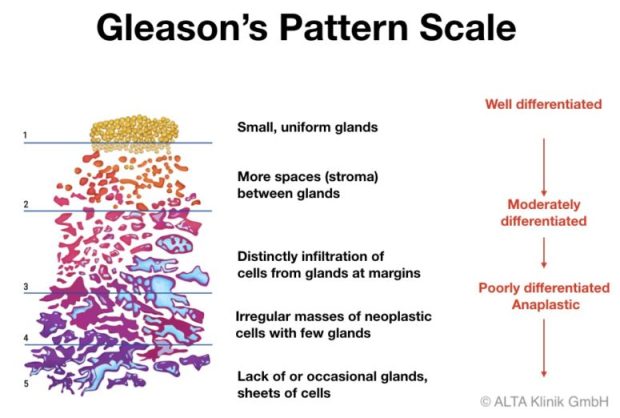
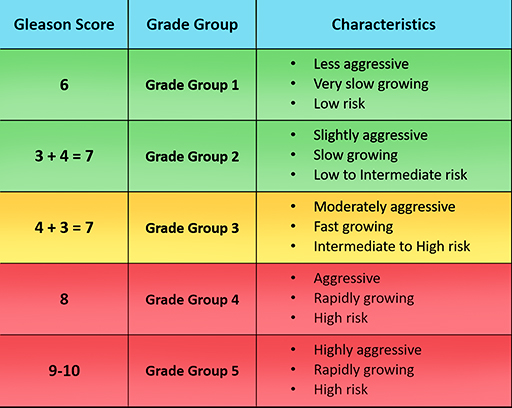
Unfortunately, about 30% of biopsy samples are incorrectly graded. One of my samples ended up being incorrectly graded as a far more aggressive cancer than it actually was. This is a really big deal. The most common Gleason scores are 3+3=6, 3+4=7. 4+3=7, and 4+4=8. Each of these different grades call for different treatments.
A Gleason 6 probably does not need immediate treatment. Those cancers generally don’t spread. Treatment is warranted on a Gleason 7, but there is a large difference in options between the two different types of Gleason 7 cancer. Some low volume 3+4 Gleasons can be watched with active surveillance. Your doctor will not want to use that approach with a 4+3.
The Gleason 4+3 and 4+4 cancers will generally involve hormone depletion for six to 24 months in addition to surgery or radiation.
If your Gleason 3+4 is misgraded low, you might fail to treat a cancer that may soon spread. If it’s misgraded high, you might undergo a lot of suffering with two years of unnecessary testosterone depletion.
You want to get a second opinion on your Gleason Score Grades. As I mentioned, one of my lesions was initially graded as a 4+3=7 when it was actually a 3+4=7.
PSMA PET Scan- After you get a diagnosis of prostate cancer, you’ll want to get a PSMA PET Scan to see if the cancer has spread. This scan is the most sensitive option and will tell you exactly where your cancer is located. Previously, detection of metastases was made based on bone scans or MRI. The PSMA PET is generally better than both of those other modalities.
Do not consent to any treatment until you are sure you know if your cancer has spread. Once the cancer is outside the prostate gland, all the focal treatments (and maybe prostatectomy) are no longer viable treatment options.
Treatment- All these tests lead up to treatment options. Use the resources I listed below to determine which option will work best for your condition and lifestyle goals. Please be cautious when evaluating side effects of these treatments. “Erectile Dysfunction” and “Urinary Incontinence” are generally defined differently than your expectations in the studies that you will be reading.
Before prostate cancer treatment, if I couldn’t maintain an erection adequate for sexual intercourse, I would be diagnosed with erectile dysfunction and proscribed a pill like Viagra or penile injections. After prostate cancer treatment “erectile dysfunction” is assumed. Very few men get normal erections back. After treatment, the researchers don’t consider it “erectile dysfunction” unless the pills and/or injections fail. So when you read something like 70% of men will regain erectile function after surgery or radiation, understand that means “with Viagra or injections.” It doesn’t mean 70% of men will go back to normal pre-treatment sexual function.
The same issue comes up with “urinary incontinence.” After prostate cancer treatment, researchers don’t define you as incontinent so long as you use one underwear diaper pad or less per day. Some leakage is expected after treatment. When you read “85% of men will regain continence after surgery” understand that doesn’t mean that you will be completely dry. I’ve found that surgeons and radiologists universally understate the negative side effects of treatment.
Also understand that your doctors are likely to recommend the treatment that they personally perform. Urologists usually recommend surgery. Radiation oncologists recommend radiation. Beyond that, the radiation recommendation will also depend on what machine the radiologist has in his office. Most oncologists recommend the standard prostate cancer radiation that consists of 40-45 daily sessions of radiation. Those radiation oncologists usually won’t tell you that protocols using 20-26 sessions of radiation have equal success rates and side effect profiles as the standard 45 dose version.
The newer MRI-Linac radiation is delivered in an MRI machine for accuracy. Most prostate cancers are treated in five sessions with this radiation and it has much more sensitive margins than the older machines. If I chose radiation, I would probably choose that method or one of the newer brachytherapy protocols. Many radiologists don’t recommend those treatment options because they don’t personally perform the brachytherapy surgeries or have access to the newer MRI-Linac machines.
After your doctor gives you his preferred treatment option, get at least one second opinion. Use the resources below to contact Dr. Scholz and/or Dr. Kishan from UCLA. Dr. Scholz will offer personal review of your case and consultation for a few hundred dollars. Dr. Kishan will do the same thing from UCLA and will bill your insurance for a telehealth appointment so you don’t have to fly to California. If I was starting this process again, I would consult with both of these men before considering any other treatment option.
Don’t panic. You have time. Most men decide on a course of prostate cancer treatment in less than two weeks without ever receiving a second opinion. That’s the wrong answer. My doctors told me I had less than two years of life remaining in 2020. When my cancer spread in 2024, I was again given two more years to live. I’m still going strong 6.5 years later. You have time to wait a couple months to get a good second opinion.
Prostate Cancer Resources
Prostate cancer: a PSA on PSA
Before we get too deep, here is Dr. Peter Attia’s masterful article on PSA, prostate cancer screenings, and the next steps if your PSA level is too high.
Newly Diagnosed with Prostate Cancer: What You Need to Know
This article and Prostate Cancer: Questions Every Newly Diagnosed Man Should Ask His Doctor are two excellent short form articles on Medium that contain a lot of very high quality introductory information. The author is a physician and prostate cancer survivor with whom I’ve corresponded.
Many Men Chose The Wrong Prostate Cancer Treatment: Here’s Why
If you prefer your information in video form, here is an excellent short form video discussing primary treatment options and why you might choose one modality over another. This one covers active surveillance, radiation therapy, and radical prostatectomy. Unfortunately, it does not include focal treatment options like TULSA, HIFU, and Cryoablation.
ZERO Prostate Cancer Support Community

An exceptional site that operates like an old-school internet forum. The quality of information is very high and the site will send you daily email updates notifying you of new articles, videos, and posts.
The Key to Prostate Cancer: 30 Experts Explain 15 Stages of Prostate Cancer
I’ve read dozens of prostate cancer books since my diagnosis about six years ago. This is by far the most useful of the lot. It breaks a very complicated process into very simple action steps and provides all the advice your doctors don’t have time to give you.
Superman’s Adventure With Prostate Cancer: One man’s navigation through the twists and turns of treatment for advanced prostate cancer
One man’s personal journey through advanced prostate cancer treatment. The book is a quick read and the author writes in a very humorous and vulnerable manner.
Prostate Cancer Research Institute YouTube Channel

If you like getting information in a video format, this is the best YouTube channel I’ve found.
Die Wise: A Manifesto for Sanity and Soul
After hearing the author speak on a podcast interview, I had to read his books. This guy operates at an intellectual level that I find hard to even comprehend. He’s definitely one of the smartest people in the room and he has some ideas about death that mesh seamlessly with some of the Amazonian shamanic practices I’ve experienced.
If you are a part of the industry the author refers to as “the death trade” (anyone who deals with or cares for dying people) or are contemplating how what you want your own death to look like, you need to read this book. It changed my views on the subjects of death and dying.
Living While Dying: My Cancer Journey
I don’t think this is the best prostate cancer reference. In fact, the author got a few of the cancer specific details somewhat wrong. Where this book shines is in recognizing how terrible the cancer treatment process is and how if the author can make it through, you can too. Everything that could possibly go wrong with the author’s case went wrong. Dude just kept getting relentlessly slammed no matter what he did. But he’s still here despite all of the challenges.
Dr. Patrick Walsh’s Guide to Surviving Prostate Cancer
A very comprehensive and informative 450-page book covering all aspects of the disease process.
The most comprehensive and current book on the market describing all the options for ADT as well as their physical and psychological side effects.
A humorous and extremely well written account of a physician’s 30-year fight with prostate cancer and his courage to reject some of his doctors’ advice in order to experiment with new treatment strategies and optimize his quality of life.
This One Episode Will Change How You Think About the World & Your Life (From #1 Cancer Surgeon)
While this one isn’t specific to prostate cancer, it’s about cancer patients in general and discusses ways to optimize your mental state when going through such a difficult time.
The men who do the best after a prostate cancer diagnosis are those who have close relationships with family, romantic partners, and friends. This book is written for those people and covers how best to support the patient you love.
Intimacy After Prostate Cancer
A weekly Substack article written by a psychologist and prostate cancer survivor. The articles are for men and couples navigating life after prostate cancer—especially the parts that are rarely talked about: intimacy, confidence, identity, communication, and emotional recovery.
I hope these tips and resources are useful for you. Please share them with the men in your life who are dealing with this condition. As I find more useful references in the future, I will add them to the article



 NSN: 1240-99-984-0230")
